TREATMENT OF ELECTRICAL
HYPERSENSITIVITY BY HIGH-DOSE, BROAD-SPECTRUM ANTIOXIDANTS AND PULSED MAGNETIC FIELDS.
Per-Arne Öckerman, M.D., Ph.D.
Emeritus professor of Clinical Biochemistry. S-430 94 Bohus-Björkö, Sweden.
Introduction.
Electrical hypersensitivity (ES) is a condition characterized by
reactions to electrically active equipment such as computers, TV, fluorescent lamps,
house-hold equipment, mobile phones, etc. The mechanism by which such reactions are
induced is not known. Certain properties of electric or magnetic fields (EMF), induction
of a hypersensitivity to EMF by chemicals or some psychological reaction have all been
advocated. The symptoms are very varied: Often only skin symptoms in an early phase, such
as redness and itching, but later also general symptoms, such as malaise, fatigue, pains,
mood disturbances, memory and concentration difficulties. A few patients have to go to
extremes in order to avoid exposure and must live far away from others in a house without
electricity. This means they are unable to have normal social contacts, go to shops,
libraries or to work. Even patients with a lesser degree of sensitivity have to restrict
their lives in order to avoid such exposure that can induce symptoms.
There is presently no generally accepted objective diagnostic
procedure for ES.
A diagnosis, therefore, can only be made by interpreting the
information given by the patient.
The most important treatment is to avoid exposure. Several other
treatments have been tried, so far with limited success only. Most patients will after
some time experience a certain improvement, probably due to a better control of exposure.
Since most people do not get ES, even when heavily exposed to
EMF, it can be presumed that there are additional factors in ES patients making them
hypersensitive to EMF. Among factors that have been discussed are chemicals such as
mercury from amalgam fillings and brominated flame retardants from new computers as well
as psychological mechanisms, such as a Pavlovian conditioned reflex.
In an earlier study it was demonstrated that exposure to an EMF
active environment increased the activity of free radicals in ES patients, but not in
healthy controls (1). Counteracting the free radical activity by antioxidants gave rise to
a significant clinical improvement (2). In the present study these findings have been
followed up. High-dose broad spectrum antioxidants have been used in combination with
pulsed magnetic fields in order to improve further the protection against free radicals
and improve cell function by compensating lack of energy.
Materials and methods.
Patients
Diagnostic criteria:
Patients were accepted if they considered themselves ES and if they could give a
reasonable description of why they did this. There were 1 male, age 29, and 33 females,
age 30-63. All had had their ES for at least 6 months, some for several years. All had
earlier tried various ways to improve with varying success.
Analyses
Analysis was made at time zero and after two months of treatment of clinical symptoms,
erythrocyte fragility (free radicals) and mobility of white blood cells.
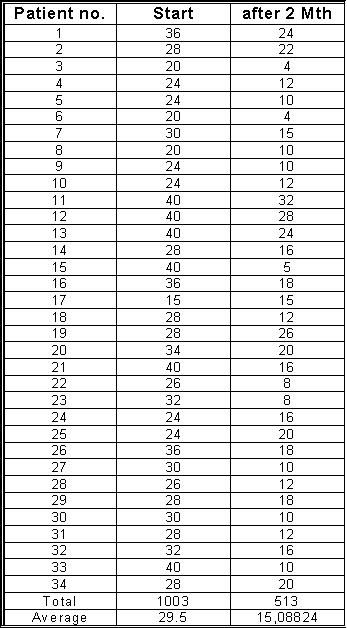
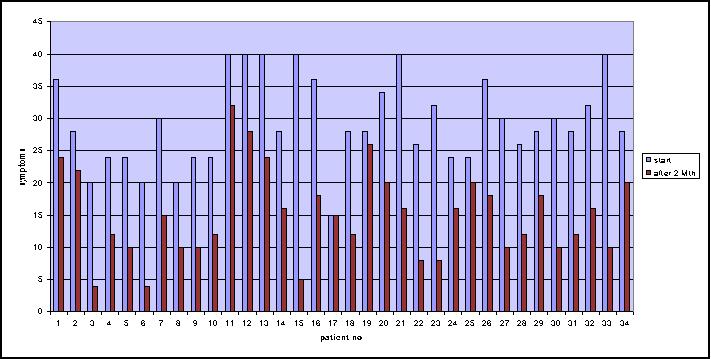
Clinical symptoms
were estimated by the patients themselves according to a subjective scale: zero
indicating no symptoms at all and ten indicating extremely severe symptoms. Values were
noted for each six hour period of the day and night. Highest possible score for a 24-hour
period was 40 arbitrary units.
Free radical activity
was estimated as damage to erythrocyte membranes by a method described in detail
elsewhere (1 and 3). An arbitrary scale was used from 0 ( no damage) to 5 0 (maximum
damage).
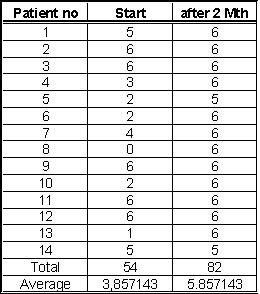
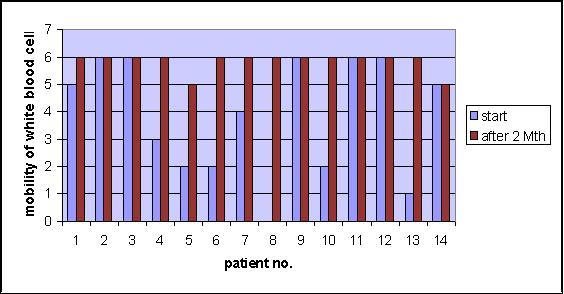
Mobility of white blood cells
was estimated on fresh capillary blood in dark-field microscopy. Full, normal activity
was called 6 arbitrary units. For this was required the existence in most cells of a
clearly visible activity in the form of movements of the granulae, vesicular changes of
the membranes and change of the form of the cells. Zero units denoted that all cells were
completely inactive and had a stable, circular form. A more detailed account of the scales
used is given in table A.
Treatment
Treatment was given by antioxidants, pulsed magnetic fields, minerals, acetyl-cystein,
melatonin and gamma-Iinolenic acid.
Antioxidants involved two different preparations:
- Polbax (Pharmacia-Upjohn-Allergon, S-262 92 Ängelholm, Sweden), 7
tablets. This is an extract from pollen, not containing pollen grains, proteins or any
material from bees. lt is a registered preparation and has been shown to have strong
antioxidant properties (4). The dose given in the present study was 200 % of the dose
recommended on the package for the consumer and slightly higher than the dose used in ref.
4.
- Antioxidant-Professor Öckerman, giving the following daily doses: beta
carotene 50 mg, vit. A 8750 IU, vit. B-1 175 mg, vit. B-2 25 mg, vit. B-3 60 mg,
pantothenic acid 175 mg, vit. B-6 120 mg, vit. B-12 0.60 mg, biotin 3.0 mg, vit. C 600 mg,
vit. D 600 IU, vit. E 350 mg, inorg. selenium 375 ug, organic selenium 120 ug, chromium
450 ug, zinc 18 mg, copper 1.8 mg, manganese 28 mg.
Pulsed magnetic fields by IMIS
(Ion Magnetic Induction System) was given on 10 - 12 occasions. Each treatment involved
liver, spleen, stomach, intestines, kidneys, thymus and neck for altogether 30-36 min. For
details of IMIS, (including address) is referred to ref.5.
Minerals
were given in the form of Cellbalans (Carls-Bergh Pharma AB, 402 58 Göteborg,
Sweden), 5 tablets. This is also a registered preparation, giving the following daily
doses: calcium 320 mg, potassium 370 mg and magnesium 170 mg. Cellbalans was given to
counteract possible deficiencies and to promote alkalinity, since many individuals tend to
have a diet that is more acidic than optimal.
Acetyl-cystein, 200 mg three times daily, was given to promote liver function
(detoxification). lt is a registered drug.
Melatonin, 3-6 mg was given at bedtime. Medication was discontinued after 2
weeks, if sleep was not improved. This is also a registered drug.
Gamma-Linolenic acid was given as Superglandin (Internordic AB, 216 22 Malmö,
Sweden), 3 capsules, containing 1.8 ml of oil from Borago officinalis, of which 25 -26 %
is gamma-Iinolenic acid. Superglandin is a registered preparation and was given in order
to promote production of anti inflammatory prostanoids.
Results
All patients completed the full treatment without side-effects.
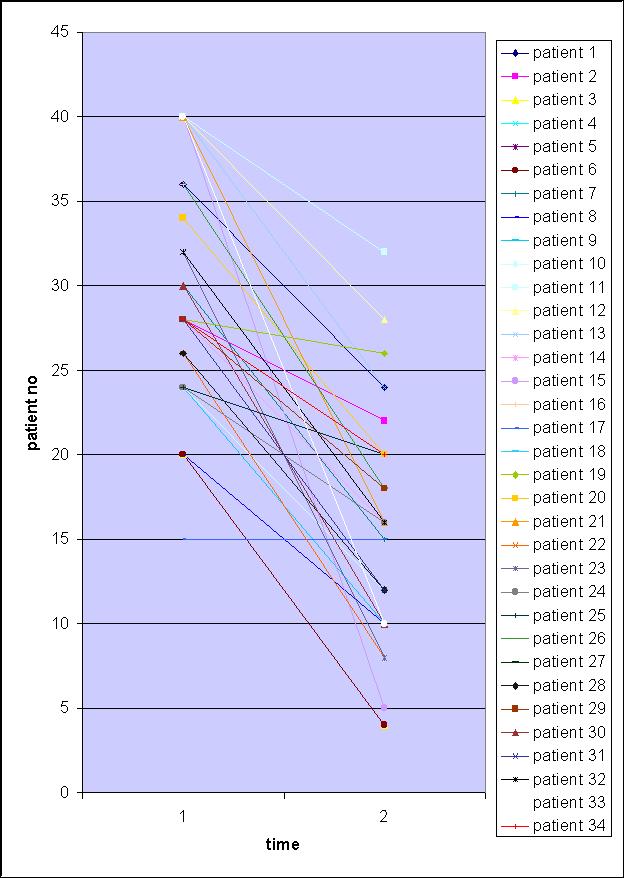
Subjective well-being improved highly significantly from severe symptoms to slight
symptoms, as shown in table 1.
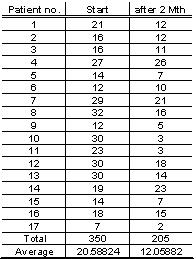
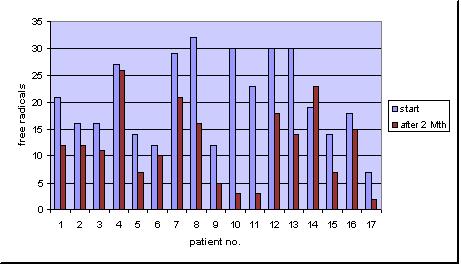
Erythrocyte fragility improved significantly, i.e. there was a
significant decrease from moderate to slight of the damage caused by activity of free
radicals (table 3).
Mobility of white blood cells also improved significantly from a
moderate decrease to normal (table 2).
Discussion
Treatment of ES has hitherto mainly been directed towards psychological
methods, in the supposition that ES actually is a somatisation syndrome. Success has been
quite limited according to preliminary results cited in an official communication by the
Swedish National Medical Board (6). The best results have been obtained by modifying the
electrical environment (6).
Earlier results demonstrated damage to erythrocytes by free radicals
through EMF exposition in ES patients, but not in controls (1). From this it might be
concluded that treatment by antioxidants could be of value in such ES patients, where an
increased activity of free radicals had been demonstrated. Support for this statement also
comes from a pilot study using a broad-spectrum antioxidant preparation (Polbax) in high
dose(2).
Side effects are in my experience rare with the preparations given in
the present study. There is one exception: some patients do not tolerate the doses given
of selenium. There was no such case in the present series. What was much more worthy of
note is that the patients tolerated IMIS. This equipment gives four magnetic pulses per
second, each pulse about one microsecond. The fields have a very broad spectrum of
frequencies, from about 150 kHz to about 250 MHz and are about 10 000 times stronger than
those coming from an ordinary PC or the computer in the IMIS.A few ES patients had stated
before this study that they did not tolerate the IMIS equipment. However, after the whole
equipment had been isolated by a copper net with no measurable fields reaching the
patients from the equipment, except the pulses, all patients tolerated the treatment by
IMIS.
In a study like this, where several different components are given, it
is, of course, not possible to state the effect of each individual component. Nor was this
the primary aim, but rather to improve the possibility of finding a more effective
treatment by combining several presumably effective components.
A large number of diseases are not caused by one single factor. Rather,
they are multifactorial. lt is, therefore, to be expected that treatment also must be
multifactorial in order to be effective. This fact makes the double-blind technique less
suitable as a tool in treatment studies and other methods must be applied, as in the
present study. This has long been accepted in e.g. nutrition. lt can be foreseen that more
complex study techniques will be used in the future also in the treatment of
multifactorial diseases.
From the results here presented it can be stated that the treatment was
quite successful and it could, therefore, be used in combination with improved
exposure control and, maybe, other methods to improve the situation for ES patients.
Knowing the situation of many ES patients, it can be stated that this is something that is
badly needed.
Acknowledgements
Financial support was given by Föreningen för EI- och
Bildskärmsskadade i Västra Sverige and by Cancer och Allergifonden.
Summary
Thirty-four patients with electrical hypersensitivity were treated for
two months by a combination of high-dose, broad-spectrum antioxidants, pulsed magnetic
fields, minerals, acetyl-cystein, melatonin and gammalinolenic acid. Highly significant
improvement was noted for symptoms, which decreased from severe to slight, as measured by
self-estimation. Free radical activity as measured by erythrocyte fragility decreased
significantly from moderate to slight. Mobility of white blood cells as measured by
dark-field microscopy improved significantly from moderately decreased to normal.
References.
1. Öckerman
PA.
Free radicals in electromagnetic hypersensitivity. A simple and sensitive method for assay
of damage to erythrocytes caused by free radicals. In manuscript.
2. Öckerman PA.
Antioxidant treatment in electromagnetic hypersensitivity. In manuscript.
3. Öckerman PA.
Monitoring free radicals by the erythrocyte fragility test. 5Ih Annual Symposium on
Complementary Health Care. Exeter, UK, Dec. 10 -12, 1998.
4. Krotkiewski M, Belboul A, Palm S, Brzezinska Z, Liu B, Roberts
D.
The effect of SOD-active plant substance (Polbax) on oxygen free radical (OFR) generation
and blood cell rheology. Clinical Hemorheology 1995; 15: 641-647.
5. Ion Magnetic Induction System. http://www.jason-health.com
6. Socialstyrelsen. Kartläggning av behandlingsprogram för
personer med elkänslighet. http//www.sos.se
|